What are common injuries seen around the wrist?
Perhaps the most common injury we would see are fractures of the distal radius (wrist) which presents after a fall landing on the outstretched wrist. This leads to a break or fracture of the end of the long bone of the forearm (radius) with deformity. Several types of fractures can occur; there can be a simple crack (fracture without displacement) that does not involve the joint but involves the end of the bone, and if they move (displace) they can either angulate forwards (Smith’s fracture) or backwards (Colles’ fracture). Fractures can also go into the joint (intra articular fracture). The aim of treating all of these fractures is to make sure the bone is in appropriate alignment so that the bone can heal in an acceptable position and not limit function or be deformed, which can lead to early arthritis.
How are these fractures diagnosed?
Fractures are diagnosed on the basis of the history and examination confirming tenderness at the site of the forearm. Following an appropriate assessment, x-rays will easily identify most fractures. If there are concerns, CT scans or MRI scans may be required. CT scans are often used to assess the shape of the fracture and how displaced the bones are, as these scans are better for demonstrating bone configuration and can produce 3D images. If there is uncertainty whether a fracture exists, an MRI scan is excellent at identifying a fracture as this will show any fluid that occurs around the bone. It can also be used to check if there are any ligament injuries.
However, this can also overdiagnose a fracture as bone bruising itself will also demonstrate as fluid. Once the diagnosis is made, we need to assess whether the fracture is in an appropriate position. The distal radius is particularly sensitive to loss of position as any shortening or angulation will put stress on the articulation between the radius and ulna (joint between the two bones of the forearm). This is important as any distortion to this will lead to inability or difficulty placing the wrist into an upward or downward position. If the break enters the joint of the wrist that can lead to distortion, stiffness of motion or more importantly it can put stress on the wrist, leading to early arthritis. Thus, it is important to get a fracture into an acceptable position.
Often the break has not moved and is appropriately positioned, in which case it is treated by an immobilisation device. This can vary from a simple plaster consisting of either plaster of Paris or fibreglass, progressing to removable splints ( which can be fitted by Full Circle Hand therapy who work in Glenelg Orthoparedic premises). These are more expensive but have the advantage being able to be removed to wash the hand or care for the skin. If, however, the fracture has moved, then it will need to be reduced into an acceptable position by either manipulating the break or a surgical procedure to align the bones. In both cases these are done under a general anaesthetic.
Usually a manipulation requires fixation with either wires or, more commonly, a metal plate holding the fracture configuration in a stable position. This has the added advantage of not having to rely on a plaster and allows mobilisation, thus reducing stiffness long term.
What other fractures occur around the wrist and hand?
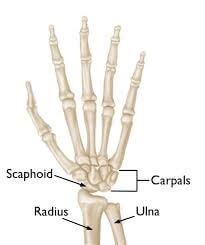
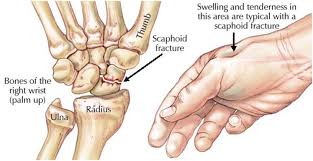
A common fracture involves the scaphoid, which is the bone that links the two rows of small bones in the wrist together and which could be considered the main “drive shaft” to wrist motion. This bone has poor blood supply because of the amount of joint surface it has, and therefore this bone has reduced healing potential and breaks can be serious. Fractures of the scaphoid often do not heal and as such whilst undisplaced fractures can be quite appropriately treated in plaster, they often require a longer period in plaster and the patient is encouraged to reduce activities that may limit the healing potential of the scaphoid, such as smoking.
In scaphoid fractures that are displaced, it is important to get the bone lined up into an appropriate position and often screw fixation is warranted, carried out under a general anaesthetic.
Other common fractures or breaks that occur in the hand are those of the fingers, known as the phalanges. These may require a plaster but sometimes require wire fixation or insertion of small plates.
The difficulty with all wrist and hand fractures is that the diagnosis is often missed. It is very common for a footballer to have a fall and injure their finger and to feel they have only sprained it. If the symptoms are not settling over a few days we would strongly recommend an x-ray to assess, as in our experience these breaks are more common than previously thought and may require treatment.
What are the risks of fracture treatment?
No matter what technique of fracture treatment is undertaken, there is always a risk that the break may move and as such any fracture or break requires regular x-rays to make sure there is no loss of position. This is more important with those that are being treated purely with a plaster.
Despite the position being maintained there is always a risk of the break not healing and this can occur whether or not there has been surgery to hold it in an appropriate position. Some patients are more likely not to heal. Age affects healing, as does health factors such as smoking. As such, all patients should be encouraged to stop smoking when they have a fractured bone. If the fracture does not heal it may require further surgery and in this scenario a bone graft may be warranted.
In the case of surgery, there are risks that need to be considered. Firstly, there are nerves close to the site of breaks, which have a very small risk of injury. This is rare and extreme care is undertaken to protect any nerves around the break.
Secondly, when metal is inserted into the body there is always a risk of infection and as such antibiotics are given at the time of the surgery. The patient will need to take care of the wound afterwards to make sure it is not exposed to anything that could increase the risk of post-operative infection. Finally, the metal might become symptomatic or prominent and may require removal at a later date, but in most cases we tend to leave the metal in place.
Finally, no matter how a fracture is treated, there is the risk of the development of secondary arthritis. Trying to reduce the fracture to an appropriate position reduces the risk of arthritis, but after any injury to a joint there is extra stress put through the soft tissues around the area which increases the risk. Reducing the alignment of the bones into the correct anatomical position reduces this risk, however there is still a long term risk of arthritis developing. This may require further treatment at a later time.
At Glenelg Orthopaedics we have vast experience in limb fractures and we would be happy to provide advice and treatment for such.
Read more about wrist conditions and treatments or contact us for advice about your specific condition. When it comes to wrist fractures and hand fractures you can rest knowing that at Glenelg Orthopaedics, we will provide you with quality orthopaedic care.