
Rotator Cuff Injuries
and Arthroscopic Rotator cuff repairs:
Rotator cuff injuries or tears are extremely common, and 1 of the commonest conditions treated by Dr Gavin Nimon. The tears can be partial rotator cuff tears (thinned out) or all the way through the cuff ( full thickness rotator cuff tear ) with the size varying from a few mms in size to most of the cuff 3-4 cm in size.
The rotator cuff is a group of four tendons which encircle the shoulder and provide stability. They also provide fine motor movements, they support the shoulder for any motion of the upper limb and stabilise the ball in the socket (humeral head in the glenoid) for all activities of use.
The shape of the shoulder is provided by the deltoid which covers the rotator cuff and provides the main motor power for the shoulder. The Deltoid is the muscle that is incorporated when doing heavy activities but the rotator cuff and the four tendons in the rotator cuff provide fine movement.
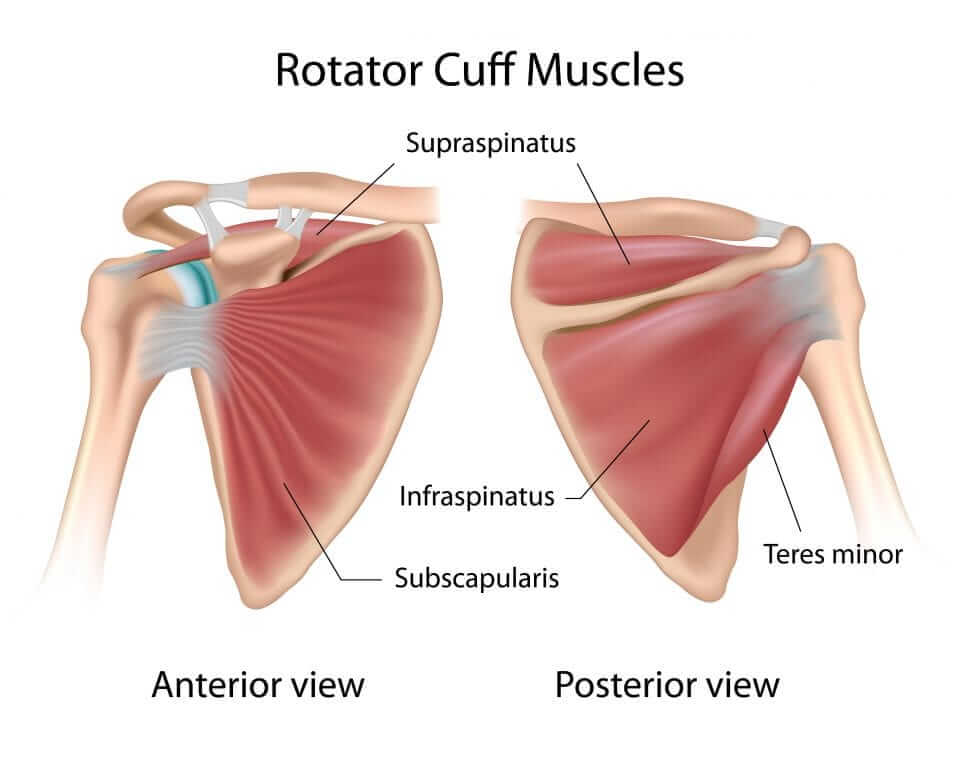
The rotator cuff consists of four tendons, the supraspinatus, infraspinatus, subscapularis and the teres minor, are used with fine motor movement, including the use of a computer mouse on a desk or co-ordinating the hand positioning to play a tennis shot. The supraspinatus and subscapularis in particular are important in stabilising the shoulder and also are at risk of degenerating and tearing. Tears occur through excessive use of the tendon and also are associated with ageing as all tendons can degenerate with age. Factors that contribute to ageing, such as smoking, are also significant factors. The tendons have a limited blood supply, preventing a good repair response, and thus with ageing tears occur naturally and are often compensated by the tendons around it so that not all tendon tears need to be repaired. If however a tendon tear becomes symptomatic or occurs abnormally early, ie in a young person secondary to either excessive sporting activities or trauma, then a repair may be warranted.
What sports are commonly associated with rotator cuff injuries?
These sports that particularly cause tears are those that involve overhead activity such as tennis, in serving there is excessive force put through it, volleyball, swimming and basketball. During the winter months Australian Rules Football can cause rotator cuff tears, although the more common injury with this is actually dislocation, which is a different scenario.
What symptoms do people develop with rotator cuff issues?
The common symptom is pain which is experienced, felt laterally down the arm, ie from the tip of the shoulder radiating laterally down towards the elbow. It is worse with movement, in particular movement above about 70-80 degrees of flexion or on attempting to lift the arm up and improves at full range of motion, in other words there is a painful arc between the 60-70 degree range up to 120 degrees. Often there is pain which is unremitting at night and can cause people to lose sleep but at rest during the day without using the arm, the pain is minimal. Often people will report symptoms of a grabbing sensation when they go to lift their arm up or when they are straining at 100% capacity in sporting activities the symptoms become prominent.
What are the treatment options for rotator cuff issues?
The vast majority of rotator cuff symptoms can be treated with rest, anti-inflammatories and avoiding the inciting factors, ie things that cause discomfort. If this fails to settle over a two to four week period then a course of physiotherapy, working on strengthening the muscles in a painless fashion using low resistance Theraband (rubber bands) is appropriate. On occasions, steroid injections are useful which will help hasten the recovery and up to three injections can be given over a six month period. If after three to six months the symptoms have not improved then it is worth seeking the advice of an orthopaedic surgeon, who would advise regarding surgical options.
What surgery is available?
The surgical options really involve an arthroscopic (keyhole) inspection of the joint and the subacromial space (the external surface of the tendons) to ascertain if there is bone catching on the tendon to inflame the tendons in certain positions. In such cases a clean out of the inflamed bursa (debridement) and decompression (removal of excess bone) is undertaken. This is not dissimilar to undergoing an arthroscopy of the knee in that it is done through three small 1cm incisions but does involve a one night stay in hospital.
Recovery can take three to four weeks before symptoms are slightly improved and can continue to improve up to three to four months or longer, depending on the person’s circumstances. In general though a person with classic features and signs of rotator cuff would expect a significant chance of improvement.



Are there any tips to prevent rotator cuff injuries?
Rotator cuff injuries can be prevented by:
- strengthening the shoulder in a steady and regular fashion rather than undertake a full regime immediately,
- avoiding excessive overhead activities and as with all exercise regimes,
- doing things in moderation, slowly increasing as comfortable but not using excessive weights; or
- undertaking excessive activities suddenly.
What conditions can be confused with rotator cuff or can occur around the shoulder?
Other common conditions around the shoulder include frozen shoulder, dislocating shoulders, osteoarthritis and referred pain from the neck.
Frozen shoulder is a condition associated with severe pain which is unrelenting and eventually proceeds to develop a stiff shoulder with reduced range of motion. This can be hidden by the fact that the shoulder blade (scapula) can move around the chest wall thus simulating good motion despite the actual glenohumeral joint (shoulder joint) being immobile. This condition is more commonly associated with diabetics and occurs predominantly in the thirty to fifty year old age group. It is self limiting and often improves on its own, although it can be helped with some hydrotherapy and occasional steroid injection to loosen up the shoulder. While there are surgical options for such a condition, such as manipulating the shoulder joint or releasing it, this is rarely required.
Unstable (dislocating) shoulders usually occur after an initial traumatic episode causing the shoulder to be forced out of joint. In such cases, the tissues around the socket (labrum) which add to the normal stability of the shoulder have been torn or stretched, thus predisposing recurrent dislocations. Often such conditions are associated with a sporting event or traumatic event such as a fall and are more common in people who have a family history or personal history of unstable joints as there is a congenital ligament laxity issue often associated.
Whilst physiotherapy could be considered, the vast majority of unstable shoulders will continue to dislocate in the age group for which sporting activities are undertaken. As people age, however, they tend to find that sport is limited to lesser activities and therefore instability is less common but still can occur. In the case of instability surgical intervention can involve repairing the soft tissues back to the socket (glenoid) which is known as an anatomical repair, or can be supported by the use of bone grafts (Latarjet) or tendon transfers which are more commonly being used but which involve a more extensive procedure.
Arthritis of the shoulder is rarer than these other issues and occurs predominantly in the age group over sixty and can be associated with previous traumatic episodes, injuries, fractures or family history of arthritis. Such arthritis usually presents with pain felt predominantly on the front of the shoulder, constantly present, associated with stiffness and as such can look like a frozen shoulder but for which x-rays demonstrate the characteristic features of arthritis. In these scenarios a shoulder replacement is an option.
If you would like to discuss anything you’ve read today or to book an appointment to speak to Dr Gavin Nimon, please contact us.